
11th November 2025
Estimated reading time : 7 Minutes
Top Orthopedic Shoulder Surgery Coding Errors to Avoid in 2026: Boost Accuracy and Reduce Denials
As a healthcare coding and RCM expert, I know that accurate coding is the bedrock of a financially healthy orthopedic practice. In 2026, the complexity of orthopedic procedures, especially those involving the shoulder, continues to challenge even the most experienced coding and RCM teams.
I. Introduction: The Growing Need for Accurate Shoulder Surgery Coding
The demand for orthopedic shoulder procedures is surging. Driven by an aging population seeking to maintain active lifestyles and advancements in arthroscopic techniques, the volume of procedures is steadily rising. Projections indicate the global rotator cuff injury treatment market alone is on track to reach $1.24 billion by 2026, with arthroscopic repair, including arthroscopic rotator cuff repair CPT, remaining the preferred surgical approach.
However, where there’s high volume and complexity, the risk of errors increases, directly impacting revenue. According to estimated 2026 Orthopedic Coding Trends data, denial rates for shoulder arthroscopy CPT code claims—including procedures like CPT code 29827 (for rotator cuff repair)—still hover between 15–20%. These denials are often not due to medical necessity but to preventable coding and documentation mistakes, costing practices millions in lost revenue and increased administrative burden. Improving coding for procedures like CPT code 29827 is crucial for compliance and financial stability.
II. The Cost of Common Shoulder Coding Mistakes
Inaccurate CPT coding in orthopedic practices carries significant financial and compliance implications. Each denied claim, whether for a simple CPT code 29805 (diagnostic arthroscopy) or a complex total shoulder replacement CPT, triggers a cascade of administrative costs for rework, appeal, and delayed payment.
The primary confusion for coders and surgeons stems from:
- Frequent CPT Code Changes: While major overhauls aren’t annual, subtle guideline shifts and new/deleted codes (as seen in the 2026 CPT code set for other specialties) require constant vigilance.
- Documentation Gaps: Ambiguous operative notes often fail to support the most specific, high-value code.
Modern RCM strategies leverage AI-based coding tools and automated National Correct Coding Initiative (NCCI) edit checks to minimize these errors before a claim is submitted. This proactive approach ensures codes like CPT 29827 and CPT 29823 are correctly paired and supported by the documentation.
III. The 6 Most Common Shoulder Surgery Coding Errors (2026 Update)
1. Misuse of Modifier 59 (Distinct Procedural Service)
The Mistake: Incorrectly appending Modifier 59 to unbundle services that are intrinsically included in the primary procedure by NCCI edits. This is a top flag for payer audits.
Coding Example: A surgeon performs an arthroscopic rotator cuff repair CPT (CPT code 29827) and a limited debridement of a discrete structure. Because the limited debridement (CPT code 29822) is considered an integral component of almost all other surgical shoulder arthroscopy procedures, it should not be reported separately with Modifier 59.
Actionable Fix: Coders must consult the latest NCCI guidelines. Modifier 59 should only be used when an edit exists between two services that were performed at a separate anatomic site or a separate patient encounter. Automation and AI-driven RCM systems are now essential for flagging incorrect Modifier 59 use, particularly when pairing codes like CPT code 29805 (often a bundled diagnostic) with a surgical procedure like CPT 29827.
2. Incorrect Use of Modifier 22 (Increased Procedural Services)
The Mistake: Applying Modifier 22 too frequently or without sufficient documentation to justify an increased payment.
Actionable Fix: Modifier 22 is reserved for unusually complex or demanding circumstances. The operative note must clearly document the “unusual circumstances,” such as excessive scarring, morbid obesity, or severe anatomical distortion. To properly justify Modifier 22, the documentation should include:
- A concise statement of the reason for the complexity.
- Specific operative note sections detailing the extra time, effort, or risk.
3. Improper Coding of Diagnostic vs. Surgical Arthroscopy
The Mistake: Billing both a diagnostic arthroscopy (CPT 29805) and a subsequent surgical arthroscopy (CPT code 29827, CPT code 29823, etc.) during the same encounter.
Coding Example: The surgeon begins with a diagnostic shoulder arthroscopy, identifies a tear, and proceeds to perform an arthroscopic rotator cuff repair (CPT 29827). You cannot bill CPT 29805 and CPT 29827.
Actionable Fix: CMS guidelines state that if a surgical procedure is performed, the diagnostic portion is bundled into the surgical code and is not separately billable. Only report the most extensive, definitive surgical procedure performed, such as the cpt code for rotator cuff repair.
4. Documentation Gaps for Surgical Assistants
The Mistake: Missing or incomplete attestation of medical necessity for a surgical assistant’s services (Modifier 80, 81, or 82).
Actionable Fix: For compliance and reimbursement, the surgeon’s operative note must clearly state the medical necessity for the assistant. Missing documentation is a common denial reason for procedures like total shoulder replacement CPT or complex arthroscopic rotator cuff repair CPT. Ensure all necessary attestations are present and properly signed.
5. Discrepancies Between Operative Notes and Medical Records
The Mistake: The procedure title, findings, and service codes selected (e.g., CPT 29824 for distal claviculectomy vs. a procedure reported as simple debridement) do not align with the narrative in the operative note.
Actionable Fix: Implement continuous coding audits and leverage EHR integration tools that use natural language processing (NLP) to cross-reference the coded service with the operative report’s text. This ensures the correct code, whether it’s CPT 29828 for biceps tenodesis or a shoulder labral repair CPT code (CPT 29807), is fully supported.
6. Incorrect CPT Code Selection in Arthroscopic Procedures
The Mistake: Confusing the specific CPT codes for different arthroscopic procedures, leading to under-coding or non-compliance.
Coding Scenario Examples:
- Rotator Cuff Repair (CPT 29827): This is the code for arthroscopic rotator cuff repair. Do not bill it with extensive debridement (CPT 29823) unless the debridement is performed in a clearly distinct area and meets the NCCI bypass modifier requirements.
- SLAP Repair (CPT 29807): Used for shoulder labral repair CPT code (SLAP lesion repair). If a limited debridement (CPT 29822) is done, it is typically bundled unless it’s a completely separate structure.
- Biceps Tenodesis (CPT 29828): The specific code for arthroscopic tenodesis. If a full-thickness rotator cuff repair (CPT 29827) and a biceps tenodesis CPT (CPT 29828) are performed, they can be coded separately because they are distinct procedures.
Actionable Fix: Scrutinize the procedure—did the surgeon perform a limited debridement (CPT 29822) or extensive (CPT 29823)? Was it a full capsulorrhaphy (CPT 29806) or a labral repair (CPT 29807)? Always choose the most definitive, most comprehensive code that accurately reflects the procedure.
IV. Understanding Key CPT Codes for Shoulder Arthroscopy (2026 Updates)
Mastering the following key shoulder arthroscopy CPT codes is non-negotiable for orthopedic RCM success in 2026.
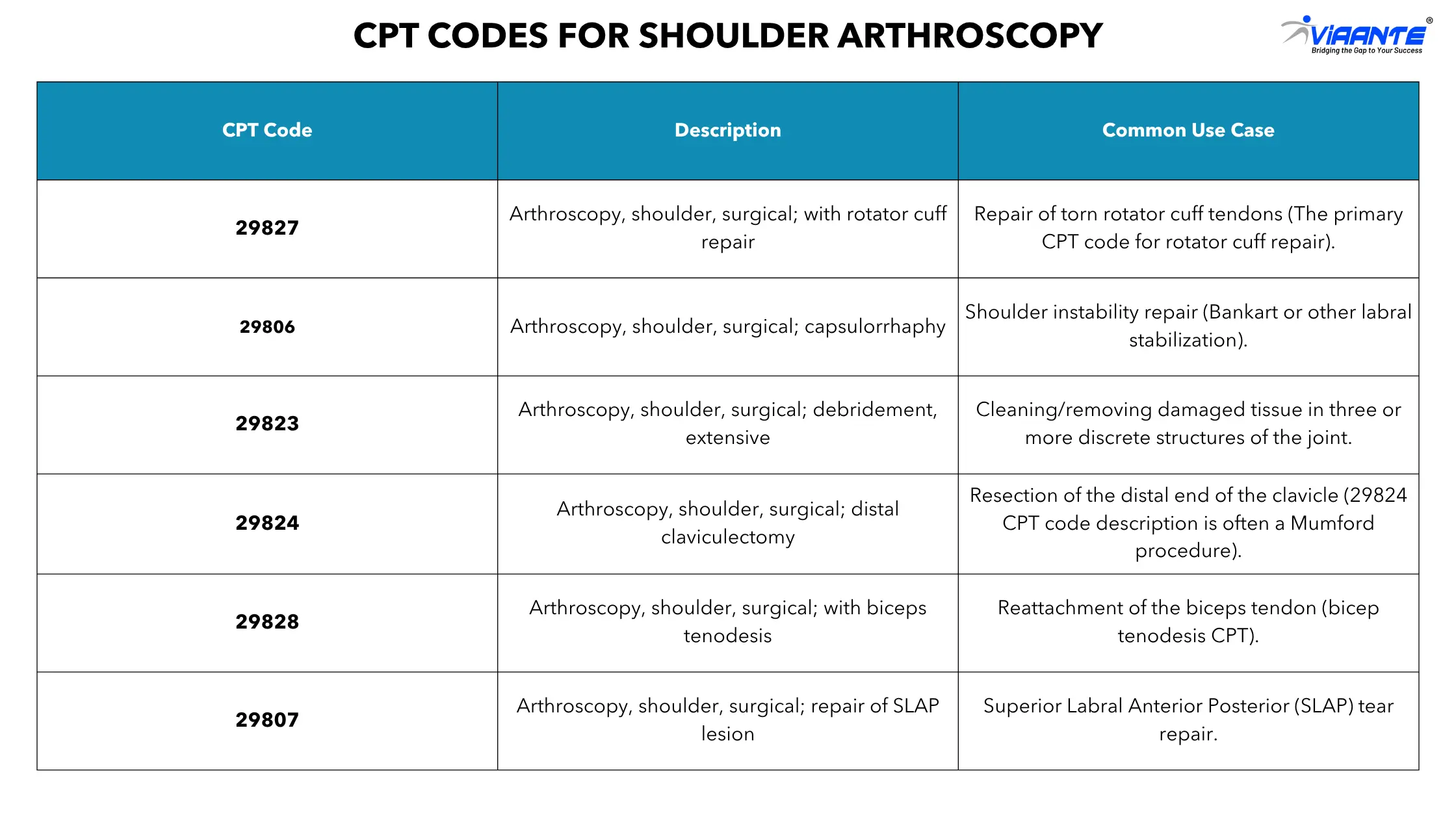
2026 Coding Note: While there are no significant descriptor changes to these codes for 2026, NCCI edits remain stringent. Codes 29824, 29827, and 29828 are exceptions that may be reported separately with extensive debridement (CPT 29823) when performed in a clearly distinct area of the same shoulder, provided the modifier guidelines are met. However, the limited debridement code (CPT 29822) remains bundled with virtually all other surgical shoulder arthroscopy CPT code procedures.
V. How Technology Can Reduce Denials and Improve Accuracy
Achieving a high-accuracy rate for complex orthopedic procedures, including CPT 29827, is nearly impossible without technology in 2026.
- AI-Driven Coding Validation: Advanced platforms automatically cross-reference the operative note with payer rules and NCCI edits in real-time. This ensures that every cpt code 29823 is justified and that the cpt code 29827 is correctly paired with supporting codes.
- Automated NCCI Edit Checks: These systems instantly flag potentially bundled services and alert coders to the required use of modifiers like 59, preventing a common source of denials related to codes like CPT 29824 and CPT 29828.
- Denial Analytics: Sophisticated RCM tools analyze denial patterns, identifying the primary payer (e.g., Medicare, Blue Cross) and code (e.g., specific issues with CPT 29806) responsible for the highest denial volume. This data allows orthopedic providers to maintain 98–99% coding accuracy by addressing systemic issues.
- Expert Outsourced Coding Support: For practices facing staffing or training gaps, outsourcing coding to certified orthopedic experts provides both temporary and permanent support, ensuring specialty-specific accuracy for high-volume codes like arthroscopic rotator cuff repair cpt.
VI. Conclusion: Achieving Accurate and Compliant Coding
Mastering the complexities of orthopedic shoulder surgery coding—from distinguishing limited (CPT 29822) versus extensive (CPT 29823) debridement to correctly applying modifiers for CPT 29827 and CPT 29807—is paramount for financial success in 2026. Continuous coding education, regular third-party audits, and the strategic adoption of advanced RCM systems are essential. By focusing on documentation specificity and eliminating the common errors detailed above, orthopedic practices can directly reduce denials and enhance revenue flow across all CPT code for rotator cuff repair and shoulder arthroscopy procedures.
At Viaante, our certified coding professionals ensure 98% accuracy, minimize denials, and help orthopedic practices maximize revenue integrity across all CPT code categories — from arthroscopic rotator cuff repair (CPT 29827) to complex shoulder arthroplasty cases.





